
Surgery in UC Hospital operating room, 1924.
Photo courtesy of: Calisphere. Collection: UCSF History Collection; Owning Institution: UC San Francisco, Library, University Archives.

For more than a century, the operating room has quietly recorded not only what surgical culture values, but also how medicine responds to uncertainty and responsibility, and holds the accumulated stories of patients whose lives unfolded there. Placed side by side, the following three images from UCSF’s past and present tell a story not of linear progress, but of continual recalibration — between surgeon and patient, between hands and machines, between closeness and distance. In a way the operating room becomes a kind of time machine, revealing how surgery repeatedly reshapes itself in pursuit of delivering better patient care.
The First Room, 1924
Photo courtesy of: Calisphere. Collection: UCSF History Collection; Owning Institution: UC San Francisco, Library, University Archives.
Surgery in UC Hospital operating room, 1924.
This photograph from 1924, taken in one of the operating rooms at the University of California Hospital (present day UCSF), is spare and almost austere. Gowned figures cluster tightly around the operating table. There is little visible technology — no screens, no computers. The patient lies at the center of the room. We don’t see the layers of imaging, specialized lighting, or digital surveillance which surround the perioperative staff today. Incisions would be larger, out of necessity. When visualization is limited and imaging nonexistent, certainty would come from exposure. To see would be to know.
We see early equipment at the edges of the room — tanks used by the anesthesia team-- and a surgeon, or perhaps an assisting surgeon, standing on a small stool for elevation, a detail that still appears in operating rooms today. The long white uniforms and scrubs differ in design between the teams present. The room itself is not cluttered, containing only what is essential. Most striking is the presence of large windows, allowing sunlight to enter the operating room — an almost nonexistent feature in many operating rooms today. The space seems more open, more alive, less compressed. Air here is not sterile in the contemporary sense, but breathing. And yet, the paradox is clear: the sealed, artificially controlled environments of modern operating rooms have been more optimal for preserving life.
The Second Room, 1968
Photo courtesy of: Calisphere. Collection: UCSF History Collection; Owning Institution: UC San Francisco, Library, University Archives.
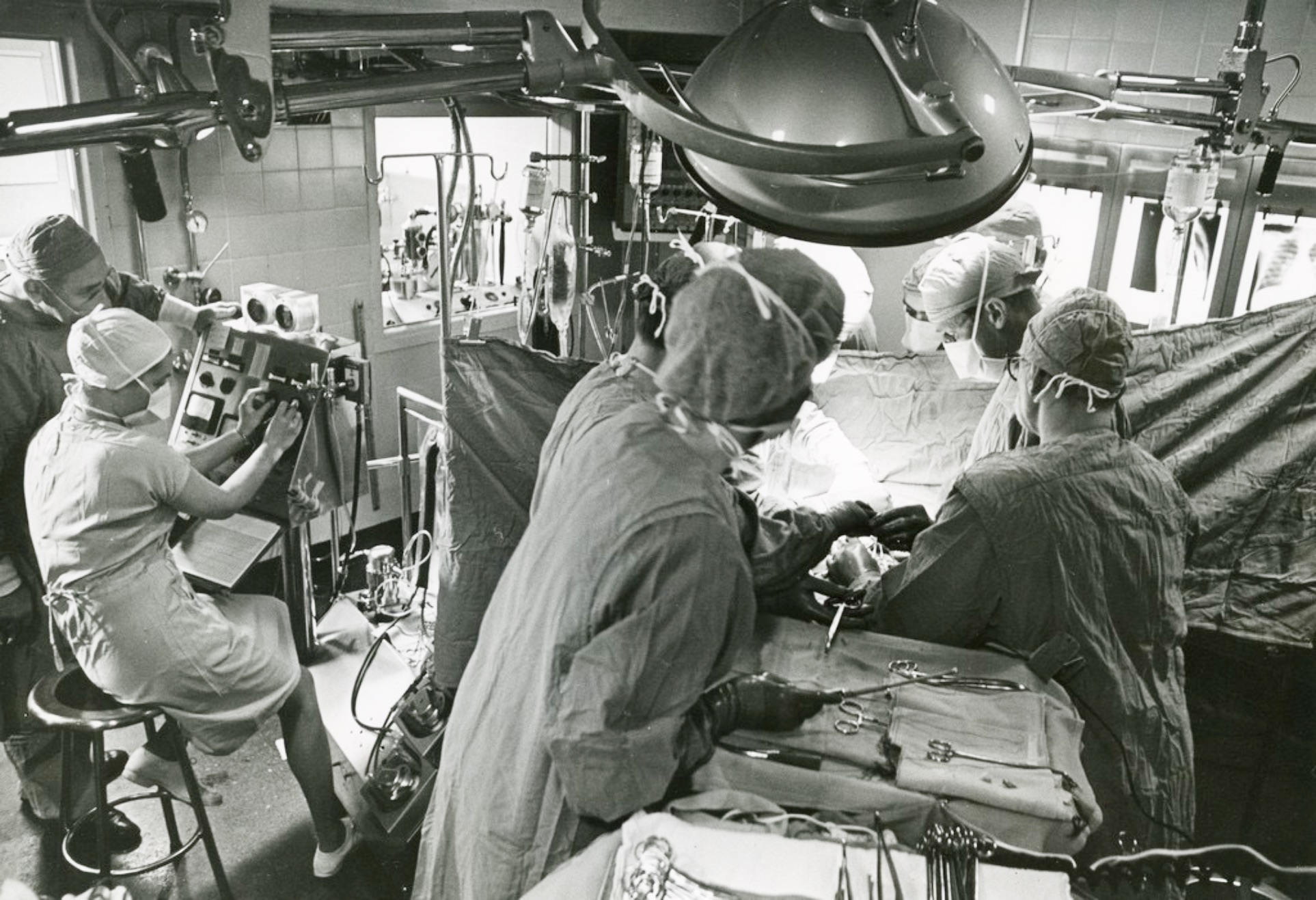
Surgery in UCSF Medical Center, 1968.
By 1968, the operating room has grown busier, denser, and louder — even in stillness. In this operating room, now at the UC San Francisco Medical Center, machines crowd the periphery, pressing in alongside the surgical team. Drapes and screens partially obscure the patient. Distinct roles emerge — anesthesia, nursing, surgery — each essential, none sufficient alone.
An anesthesia provider sits apart in the far left, monitoring equipment that demands constant vigilance. Overhead lights loom large and mechanical, no longer supplemented by daylight. Advances in monitoring and postoperative care allow surgery to expand in scope and ambition. This shift mirrors UCSF’s growing role within San Francisco’s public hospital system; trauma care, in particular, transformed surgery into a collective endeavor. Survival depended not on a single brilliant maneuver, but on protocols, communication, and timing.
The space feels more compressed, more controlled. The air is more sterile, the margins for error smaller. In exchange for this control, intimacy seems to recede. The patient seems to become partially hidden, known through instruments and signals as much as through direct sight. Surgery in 1968 reflects a turning point: no longer defined by proximity alone, it is increasingly shaped by coordination and ongoing innovations.
The Third Room, 21st century

Photo courtesy of: UCSF MedConnection, 2024.
The contemporary operating room is strikingly different. It is spacious and surrounded by screens. In this room in particular, the operating surgeon may no longer stand over the patient at all, and instead be seated at a console several feet away. Hands move, but not against tissue — rather, through interfaces that translate motion into action at a distance, in the pursuit of finer patient outcomes.
Precision increases. Tremor decreases. Incisions shrink.
Human intention now passes through robotics and instrumentation before reaching tissue. Physical proximity gives way to visual dominance. Touch becomes indirect. Anatomy appears magnified and illuminated on screens rather than directly beneath the surgeon’s gaze.
The operating room functions less as a shared physical space and more as a network — of consoles, monitors, and robotic arms that interpose themselves between surgeon and patient. The patient is present, yet increasingly abstracted, known through pixels and ports as much as through direct contact. What is gained is undeniable: less pain, faster recovery, extraordinary control. The surgeon is physically farther from the patient than in the previous two rooms, even as visual access reaches unprecedented depth.
This room does not replace the earlier ones; it contains them. It exists alongside countless surgeries that continue to be performed through open or laparoscopic approaches. The endurance of the first era and the systems of the second persist beneath layers of software, machinery, and protocol.
These photographs don’t depict a straightforward story of improvement, but rather one of repeated moments of innovation and courage — when clinicians set out to upgrade their systems and workflows, and to work toward a shared goal of advancing patient care while reducing harm. Each shift reflects an effort to honor the trust patients place in the operating room on one of the most vulnerable days of their lives, and to preserve their dignity as much as their outcomes.
Each room seems to solve the problems of its time while introducing new tensions. Early surgery demanded courage but tolerated risk. System-based surgery improved safety but required coordination and trust. Robotic surgery offers unprecedented precision while raising questions about access, cost, and distance. In that sense, every operating room is temporary — yet leaving us to ask: what are we carrying forward, and what are we quietly leaving behind?


